
he entire human race uses “language”, with the exception of the comparatively few people suffering from some sort of impairment, as a matter of course. Although there are differences regarding region/land and historical time, people in a specific location and at a specific time take the use of their “native” language for communication with other people of the same time and region for granted. While there are differences among different languages in the way how certain things/concepts are handled, the basic idea of conveying information between people is probably everywhere the same.
To quote from the Wikipedia(1):
“(language as) A tool for communication
Yet another definition defines language as a system of communication that enables humans to cooperate. This definition stresses the social functions of language and the fact that humans use it to express themselves, and to manipulate things in the world.”
Again from the Wikipedia, pertaining to communication(2):
“Human communication
Human spoken and written languages can be described as a system of symbols (sometimes known as lexemes) and the grammars (rules) by which the symbols are manipulated. The word “language” is also used to refer to common properties of languages. Language learning is normal in human childhood. Most human languages use patterns of sound or gesture for symbols which enable communication with others around them.”
Problems arise, when people of one specific region try to communicate with people in or from other regions. These problems arise already during communication related to common things like food, housing, directions etc., occasionally even among speakers of different dialects of the same language, but become much more complex in areas of high specialization. Oriental medicine is one such area. Even if one assumes, that the people who try to study and/or communicate about oriental medicine are already experts in their field, communication of specific concepts using different languages may represent a very challenging task. Assuming that there is a wealth of valuable information, which I will define for the sake of this discussion as information originating in Japan, this is and remains of very little use. That is because it is (encrypted) in Japanese, which mainly precludes access to it by most people of the world and information becomes only then really useful, if it is made available/accessible.
I am not a scholar and do not speak on behalf of any particular group of people or organization, but would like to formulate a few of my personal concepts related to this topic. In particular I would like to focus on aspects of the Japanese language, how it seems to be currently handled and understood in this field of learning and what potential future students of oriental medicine might expect or would like to see.
xxxxxxxxxxxxxxxxxxxxxxx
As stated above, language is used to convey concepts among people. This is an extremely simplified statement, but since I do not want to/can delve into all the complexities of research into language, communication and information exchange, I would appreciate, if you will permit me to leave it standing as it is.
The Japanese language is quite different from both English or other European languages and other oriental languages like Chinese. It does not use articles, rarely distinguishes between plural and singular and handles nouns and verbs differently from the way this is done in English for example(5). This may contribute to the impression, that Japanese is complicated and so difficult to learn, that most foreigners are not expected to have much success. Yet, Japanese is a highly developed, delicate and elegant language. Examples of highly refined typical Japanese literature like the “Genji Monogatari” for example, even though they use the writing system imported from China, antedate comparable works sometimes almost by centuries.
Yet, the Japanese people themselves seem to suffer from an inferiority complex about their language precisely because it seems to be so difficult and inaccessible. In a very illuminating book written by the linguist Suzuki Takao “The World of the Closed Language Japanese”(8) the author points out, that Japanese is actually one of the top 10 most spoken languages of the world. In his book he cited Japanese to be on rank 6, but while the rank has dropped to “9”(6) since its publication 30 years ago, it still remains among the most frequently, widely spoken languages of the world. There is nothing to be ashamed (shame is also a concept of special cultural significance in Japan) of. Rather on the contrary: I firmly believe that Japanese people should take more pride in their language and their achievements, which are largely expressed through this language. This in turn suggests, that materials explaining these achievements should be made assessible to the world through translation.
However, because of their fear, that other people/languages may be superior to their own and in conjunction with the aggressive promotion of a “standard TCM terminology” by the Chinese through the WHO(7), the Japanese have adopted a quite restrained behavior of promoting/displaying their own concepts and practice of oriental medicine through the use of Chinese dominated language. The result is an almost unbearable mixture of expressions, circumscriptions etc. that make even comparatively simple ideas almost unintelligible for many students of the matter throughout the world. I will try to illustrate with a few examples.
Occasionally I translate Japanese articles meant for magazines etc. that have the purpose of promoting the Japanese concepts pertaining to the use of Chinese herbal medicine, called Kampo, as well as research into acupuncture and oriental medicine in a wider sense.
Yet, while the use of Chinese herbal medicines in the Japanese way = Kampo should be considered an original Japanese application, editors sometimes/often cling to the Chinese form of an alphabetical notation of the relevant terms. For example, certain editors follow the recommendations by an authoritative academic (Japanese) society for the research into Kampo medicine and thus demand from me, that I write the name for prescriptions as ONE word, appearing in third place after English and Chinese like:
* Cassia Twig and Tuckahoe Pill plus Coix Seed
* Gui-Zhi-Fu-Ling-Wan-Liao-Jia-Yi-Yi-Ren
* keishibukuryoganryokayokuinin
Here I can understand the use of an English translation. That certainly facilitates access to this information. The Chinese notation at least shows the breaks between individual characters, facilitating search in dictionaries and possibly also provides clues about the pronunciation. While the Japanese … (12)
The above shown Japanese “word” has 29 (!) characters. There are even longer ones, like for example “yokukansankachinpihangegotokishakuyakusan” with no less than 41 characters. And, while the English and Chinese terms are treated as proper nouns and thus capitalized, in the example above the Japanese term appears only in lower letters, as if it were no proper noun.
I once asked a scholar about the necessity of expressing the Japanese terms as single words. The answer was, it would be very difficult to decide where to put any possible breaks. Again, I have great difficulties in believing, that the current approach will facilitate the declared purpose(9) of disseminating relevant information.
For example, one could easily break down the expression for the prescription called “Keishikaryukotsuboreito” in the following way:
* Keishi = drug name
* Ka = processing instruction
* Ryukotsu borei = names of TWO drugs
* To = drug form.
Not even Japanese persons would consider Keishikaryukotsuboreito” to be ONE word, even if it is ONE name. For a Japanese person the term becomes immediately intelligible by looking at its elements, in particular since the Japanese know the associated Chinese characters for this term. This latter information and the underlying structure is presumably NOT available to many possible students of the material, unless they have previously acquired a considerable knowledge of the Japanese language, and thus makes comprehension very difficult, it not impossible. This includes also the difficulties encountered during attempts of looking up the term in dictionaries, that are newly created by this notation.
When I showed terms like “ryokeijutsukantogotokishakuyakusan” to Japanese people and asked them to read that for me, ALL were struggling very hard or could not figure it out at all, although they could read, naturally, the term when it is written in Chinese characters.
A little search about the use of long words in the English language showed, that the longest non-coined and nontechnical word is “Antidisestablishmentarianism” with 28 characters and the longest word in Shakespeare’s works is “Honorificabilitudinitatibus” with 27 characters(4). So, for any “reasonable” discussion words of less than 20 characters should be suitable/comprehensible. “yokukansankachinpihangegotokishakuyakusan” (41 characters) is simply incomprehensible. The use of notations like “Thisisalonggreenhouseattheroadside” or “Lelangageestunsystme de signesidentifis permettantunecommunication entreune ouplusieursentits” would NOT help any learner of English of French respectively. Further, I believe that MOST people will have difficulties pronouncing the English word “Supercalifragilisticexpialidocious” with 34 letters, that was in the song with the same title in the Disney musical film Mary Poppins(10), without any practice.
Following the same argument, I think it would help both foreign students as well as ultimately also the Japanese practitioners, if terms related to acupuncture like “Seppi”, “Hinai Shin” etc. were left in Japanese and maybe provided with a descriptive English translation. In a similar fashion the technical terms related to Judo or other forms of martial arts are used WITHOUT translation. If the provision of such word pairs is too difficult to integrate into every text, it should be no problem at all to set up a frequently updated online database with the relevant terms.
After all, anyone who starts learning a certain subject, here oriental medicine, or a particular language, here Japanese, WILL have to refer to dictionaries and other reference materials. In this respect, with all due deference, I am under the impression that the highly educated scholars who have apparently been working on the above mentioned standard terminology or are representatives of the academic societies that strive to study oriental medicine and disseminate the relevant information, may have lost touch with basic problems learners have to face. In particular regarding the use of terminology, I firmly believe that the currently used Japanese approach is wrong.
Let’s consider the use of dictionariess for an attempt to find out more about “keigairengyoto” = Jing-Jie-Lian-Qiao-Tang.
If you use a Chinese-English dictionary that provides alphabetized entries, you will know, that you are looking at a term consisting of 5 characters and can look up each according to its reading. However, there are naturally a large number of characters reading “Jing” and in ordinary language most probably no combination like “Jing-Jie”. For that purpose you need a special dictionary.
The Japanese is worse, much worse. Here you are offered only ONE term. Even if the learner suspects, that this term consists for more than one character, HOW should this learner look for the relevant characters? The term could be split like:
* ke iga iren gyo to
* kei gairen gyoto
* keiga iren gyoto
* keigai rengyo to etc.
That gives the student many possible dictionary entries to look up – a largely futile effort.
For anyone who does not know the language (Japanese), all of the listed divisions are equally possible. Depending on how the individual terms/characters are listed in the particular dictionary, this may render a search almost impossible. If the particular dictionary does NOT provide alphabetized notations, most foreign readers are denied access to this information right from the start. I have experienced this myself many times. Unfortunately, to my knowledge there are, with one little exception(11), no proper dictionaries that would help foreign students getting access to the required information. The shortest, and only, way would always require the combined use of several Chinese-English, Chinese character, Japanese-English dictionaries. Occasionally more than one of each type.
Apart from the standard dictionaries there are a number of special dictionaries for oriental, in this context mostly Chinese medicine. Sometimes the tycoons in the field publishing those dictionaries then argue about who has the “right” translation, which will invariably be different from what is found in dictionaries published in China and among the latter ones again, each gives something different and here the English rendition itself more often than not appears to be rather dubious. What the WHO has published recently as the “agreed upon standard terminology” still feels in many instances not right, at least to me. And, naturally, that terminology assumes that everything must be based on Chinese concepts.
Since people are basically dealing with “Chinese medicine”, this consensus is of course not wrong, but what happened to the Japanese view and all those aspects special to Japan? The basic concepts of acupuncture and herbal medicine have been brought to Japan about 1,500 years ago and over centuries after that through books and by practitioners. Yet, that is a long enough period for some original, independent developments to take place. Take for example the use of guiding tubes for acupuncture: a purely Japanese invention. In conjunction with the cultural differences, climatic and geographic differences and not least the mentality of the people this period of 1,500 years of development has led, I believe, to the establishment of conceptional systems and practical applications that are clearly distinct from the Chinese form ? even though many Japanese practitioners strongly assert, that they are practicing CHINESE medicine.
In spite of the thus historically formed system of a typical Japanese approach to oriental medicine, the insistence of the people in charge to NOT make this information publicly known, or to choose deliberately expressions/notations that are/will be incomprehensible for many/most non-Japanese persons, is a waste of very valuable resources.
I do hope, and possible can help to stimulate the process to adopt a more enlightening approach to the “dissemination of information”, so that the mountains of intellectual treasures currently hidden behind the veils of the Japanese language can be more easily assessed by the people of the world.
References:
(1) http://en.wikipedia.org/wiki/Language
(2) http://en.wikipedia.org/wiki/Communication
(3) http://en.wikipedia.org/wiki/Information
(4) http://en.wikipedia.org/wiki/Longest_word_in_English
(5) An Introduction to Japanese Syntax, Grammar & Language
by Michiel Kamermans; grammar.nihongoresources.com
http://grammar.nihongoresources.com/doku.php
http://www.thejapanshop.com/
(6) http://en.wikipedia.org/wiki/List_of_languages_by_number_of_native_speakers
http://www.photius.com/rankings/languages2.html
(7) WHOIST
WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region
(8) 鈴木孝夫: 閉ざされた言語・日本語の世界 (Suzuki Takao “The World of the Closed Language Japanese”)
(9) From the JSOM HP:
“Objective:
The intention of the society is to hold research presentations and seek communication, tie-up and promotion concerning oriental medicine and contribute to the progress and dissemination of oriental medicine, and thus contributing to the development of scientific culture.”
(10) http://en.wikipedia.org/wiki/Supercalifragilisticexpialidocious
(11) Japanese-English Dictionary of Oriental Medicine; written and compiled by JONG-CHOL CYONG M.D. & Ph.D.; Oriental Medicine Research Center of the Kitasato Institute, Tokyo; ISEISHA
(12) Comment pertaining to: “WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region”:
* In this dictionary the items are listed in the order “Code ? Term ? Chinese ? Definition/Description”. “Term” represents the column with the English terms and “Chinese” lists the corresponding Chinese terms ONLY in Chinese characters. That means, users cannot search the dictionary according to reading/pronunciation of Chinese terms and MUST know, what they are looking for in English. Or else they have to read through entire sections of the book.
* The only section, that provides “pronunciation” is the one listing classical medical texts. However, this too looks to users who are NOT very familiar with the different involved languages like a deliberate attempt at making things as incomprehensible as possible:
Chinese: 素問玄機原病式 = Suwenxuanjiyuanbingshi
“Suwen” may be known well enough, but xu-an-ji or xuan-ji?
Japanese: 百腹圖説 Hyakufukuzusetsu
Should it be “pronounced” Hyakufu kuzu setsu or Hya kufu ku zusetsu?
萬安方 Man’ampo ? the approstrophe is almost a relief and very helpful!!!
Korean: 鄕藥救急方 Hyangyakgoogeupbang ? I have no idea at all how this is supposed to be pronounced!
Vietnamese: 保嬰良方 Bao Anh luong phuong ? even though I do not know how to pronounce that, I can clearly infer, that the term is made of 4 characters and look up their respective meaning, if I have Vietnamese dictionary (with alphabetical notation).
Even if the above are ‘single terms’, I am convinced that native speakers of the respective language pronounce these terms with certain intonational structure, revealing the listener clues to the makeup of the relevant terms. Without these clues, in the above example the apostrophe shows the listener/reader, that there is a break after “Man” and the term is not read Manam Po. Considering that even native speaker among themselves use these intonational structures, imagine what will happen, if someone who does not know the proper pronunciation of the relevant languages tries to read those terms / pronounce them / use them during communication with other practitioners.
Tag: WHO
医療 - 問題の多いテーマ
先日、5月14日の読売新聞に東京都医師会が一面を使って「東京宣言」を公表しました。
75歳以上の患者にちゃんと治療しますとの約束をしました。この業界の危機を象徴的表し、強い違和感を私に与えました。
先書きましたが、私は小さな鍼灸院を開業しているドイツ人鍼灸師です。鍼灸師として毎日臨床現場で「医療」を携わります。多数の患者の悩みも聞きますし、 現代医学治療の問題に間接的、又場合によって直接的「見えます」。私は学者ではないので、諸問題の解決策は提供できませんが、現在多数の問題が重なる中で もしかして思考パターン(コンセプト)を少々変えるべき時期が来たと思います。これに関してこちらの見方は参考になれば嬉しい。
1.行政
2.医師
3.医療
4.その他
行政
大分前になりますが何時か厚生省に訪れた事あります。残っている印象は:恐ろしく長く、天井の低い暗い廊下、そこから分岐する部屋。その部屋は外界と繋 がる窓もない、多数の机が無秩序で大量の(どちらかと言うと汚い)資料に覆われていました。そのような環境でお仕事をする方々は医療の現場が見えないで しょう。行政から何かの「新しい制度/決まり」が発表された、既に20数年前(私は病院で勤務していました)医療現場で働く人たち(医師、看護師など)は 悲鳴を上げました。
時々そのような新しい制度の信憑性をあげるため、大学の教授、有識者、統計学や「科学的根拠」を頼る事もあります。しかしながら、そのような情報源はやはり現場を知らないので、「雲の上」の生活を送っているのは現場の人間全員思っているでしょう。
行政的に多数の問題に関して何かの取り決めをしなければなりませんのは残念ながら事実です。ただし、現在問題が多すぎるため医療制度そのものが既に崩壊 し始めている中では、雲の上で夢を見ている方よりも、現場で毎日体をはって現在の医療制度を実際に支えている人々の声を聞くべきでしょう。
医師
医師、または医者に関して歴史的の背景もあるから、私のような愚か者は論じるべきではないでしょうが、幾つか妙な点はあります。先ず、医者だけではな く、「医者様」と呼ぶ事を良く耳にします。難しい事を勉強し、人助けに力を注いでいる人に対する敬意を表すのも結構ですが、相手が余りにも偉いようでした ら患者との「普通」のコミュニケーション (communication = share something) が旨く取れなくなることあります。「お」医者「様」が患者に如何ですかと聞いても、多くの場合患者は本音で答えないで、お蔭様で・・・との態度をとりま す。しかし、仮に病院の後に私の治療院に訪れると愚痴をこぼし、医者に対する不満を表現し、又は医者に言われた事に関して私から「解説」を求めます。毎日 のようにこのようなことが起こりますので、医者は自分と患者の間かなりの溝があるのは気づきません - 気づくはずもありません。
初心に戻って「医は病を治す工である」の精神を復活させ、国民の指導者でもあるべき医者はもう少々背を低くして謙虚になると大いに助かります。
無論その反対も同様にいえます。医師に対する患者の態度にも大きな問題あります。深刻な問題は全くないのに取り合えず病院に行こうと言う態度は改めるべ きでしょう。先ず、本人は出来ることをやってみて、それでも問題が残れば、専門家を聞けばよい。「商品のトラブルシューティング」は皆そうです。私の患者 に「主人はもうなくなったし、犬もいないから、ここに来させてください」と言う人がいます。私の治療は国民健康保険を使わないから良いですが、どこか妙な 考え方。同じ患者は日頃高血圧のためにも受診するそうです:脳神経外科に!
したがって、一方患者の行きたがる態度と一方医者が患者を定期的来させる思考(例えばちょっとした怪我の人を毎日「消毒」の為に病院に来させる)が重な り、最終的「医者依存症」を作り上げます。私のモット「患者を来させないことが私の仕事だ」は以前一度雑誌で公表されたとき患者も同業者もびっくりし、怒 られました。
医療
さて、最近単に色々な問題が発生しているだけではなく「医療崩壊」と言う概念まで発展してしまいました。それ故に上記の「東京宣言」が発表されたでしょ う。医療費が高い、介護費も高い、高齢者の割合も持続的に上昇します。時期に医療制度そのものを支えきれなくなり、崩壊するだろう・・・
それは第三世界貧困地域/社会と同様です。ご存知のようにWHOは1980年代に「HFA2000 = Health For All by the year 2000」(全世界の人々に2000年度まえ健康な生活を提供する)と言う計画が考案され、その実行の可能性を探るため色々な調査もされました。調査結果 は “Traditional Medicine and Health Care Coverage”, WHO 1983(世界伝統医学大全、1995)、R. Bannermann, ISBN: 4-582-51311-5に纏められ、出版されました。結論:現代医学(西洋医学)だけでは世界の人々に健康な生活を提供する事は出来ません!その結果 は既に25年前に明らかになりました。今日「医療後進国」(以前私が書いた文章:http://www.einklang.com/download/behind.htm) になった日本そのような25年も前の知識を目覚めなければなりません。
更に、「医療」とは裕福階級の世界にしてしまうのは決して得策ではないでしょう。つまり、医学部に入りたいにしても、先ず金銭的にかなりの余裕がないと 医学の勉強は不可能になります。そして医師になったら先ず金銭的な心配は一切要りません。先日テレビで「医療崩壊」を話題にした番組中ある医者が以前病院 に勤めたが、その仕事は余りにも大変ですから退職した。その後「フリーター」と言われる形 で仕事しました。それによって収入は以前よ りも50%上昇した:年収=6000万円、以前は4000-4500万円。それはご立派です!
年収=6000万円=月収が500万円! 私の治療院やっと年の売り上げが300万に達しました。翻訳の仕事分と合わせて年収が4-500万。しかし、親は子供を医学部に入れるためのお金があるだ けでは、卒業する医師はその素質があるとは限りません。日本は自分の医療制度に対して何らかの危機感があれば、先ず優秀の人材を作る教育課程を見直し、そ の教育費を税金(?)で賄いながら医者になる素質/人格のある人材を育てて、医師の仕事は職人の仕事だと再認識し、そして職場の労働条件(臨床-当直-臨 床=36時間勤務)をもっと人間らしくしたほうが良いでしょう。
少々脱線かもしれませんが、ドイツ語では「仕事=職業」は “Beruf” と呼びます。この単語は「”Berufung” = 召命」から由来します。もし医療従事者になるのは上記の「召命→使命 = “Berufung” =天職」だと信じるようでしたら、患者の為命を捧げて全力尽くすのは当たり前です。ただ、医療従事者も人間ですので、体力の限界は あります。無理の勤務体制の為に体を壊してしまえばこそ、患者の最大の迷惑になります。患者にそのような迷惑をかけないため、適切は休みを頂くのはどこに も悪くありません。同僚など(病院の人事部を含む!)もこの人は上記の意味で天職を従事すると分かれば、少々休んだりして批判は出ないはずです。
その他
要するに、医療、又は医師-患者関係、利用する医療手段(現代医学、伝統医学)などの概念は考え直すべきでしょう。多分医療の効率はどのようにあげられ るかを考えるのなら投薬の削減、病院のベッド数の削減、保険制度の小細工などではなく、人の治療に於いてもう少し “holistic” なアプローチをすべきでしょう。一人一人の患者をもっと丁寧に、もっと時間を掛けて診れば、最終的その患者はそんなに頻繁に来なくて済むのではないでしょ うか。
私は残念ながら「有識者」ではありません。私は単なる三流の職人に過ぎませんが、職人が学者が見えないもの必ずあります。私の声は恐らく何方にも届かな いでしょうが、ここ自己満足のため簡単に纏めたのは「拙者」の意見です。更に具体的なことは沢山言いたいが、時間と場所がないため、又別の機械に委ねた い。
医道四弘誓願:
疾病無辺誓願療
病因無尽誓願断
病理無量誓願学
医道無上誓願成
原文:
- 衆生無辺誓願度(しゅじょうむへんせいがんど) – 地上にいるあらゆる生き物をすべて救済するという誓願
- 煩悩無量誓願断(ぼんのうむりょうせいがんだん) – 煩悩は無量だが、すべて断つという誓願
- 法門無尽誓願智(ほうもんむじんせいがんち) – 法門は無尽だが、すべて知るという誓願
- 仏道無上誓願成(ぶつどうむじょうせいがんじょう) – 仏の道は無上だが、かならず成仏するという誓願)
医療の後進国日本
(download: file)
- リソースの使用がお粗末 –
多数の方々は上記の発言に対する反応は「まさか」と驚く事に違いない。しかし最先端で極めて高価の技術を利用するだけは「発達」の兆候ではない。こうした技術や科学の進歩はあまりにも輝かしいから、もう少し自然に密着している人間らしい立場を見失う事も不思議ではないが、今こそまで築き上げた文明の力を発揮する所だ。
健康と統合医療
先ず、健康に関してWHO(世界保健機関)の憲章前文では「完全な肉体的、精神的及び社会的福祉の状態であり、単に疾病又は病弱の存在しないことではない。」(“Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”)と定義されている。つまり、バランスが取れたら状態を言い、そのバランスが失われた時、全ての側面から取り戻す努力が必要だ。
このような「包括的」な観点をもつ医療は昔から医療の原点でもある。最近これが「統合医学」又は「統合医療」(integrative medicine)と呼ばれ、世界中の注目を浴びている。しかし日本に於いて相変わらず西洋医学(保健医療)と他の医療体系(例えば東洋医学)の「混合医療」は禁止されている。西洋医学に完全頼り切っている。但し、その体系は論議の余地のないほど極めて高価で高度の技術をようする。その目標を実現に当たって要求されるリソースを考えれば国民のためになるとは思えない。WHOはこの問題を既に1983に出版された ”Traditional Medicine and Health Care Coverage” (日本語版:1995「世界伝統医学大全」) 取り上げた。世界各地の人々の保健を充実したいならば、その地域や文化に従来から利用されている手段を検証し、十分の利用価値を裏付けるものなら最先端の技術と統合しなければならない。後にこう言った概念を踏まえて”HFA2000” (Health For All by the year 2000、全世界に於いて)計画が発表された。2004年現在でも実現まで至っていないし、高価の西洋医学のみでは不可能だと判断せざるを得ない。
リソース ― 人材、予算、知的財産
数多くの大病院にそれこそ多数の医師が勤めている。予約があるのに長時間に待たされた挙句の果てに実際の診察/治療の時間は僅かである事実は医師の数が足りない発展途上国と大差がないように見受ける。
ある程度(かなり)裕福の家庭出身でないと現時点日本に医学を勉強する事が難しいのは、最適の人材を育成するも困難である事を別問題にしても、次のヘッドライン(その横に「ある小児科医師の死」もあった)は貴重な人材を粗末する事示唆する。(その事は無論他の人材に関しても適応する。)過労死になるまで働かせるほど医師の数が足りないはずはないでしょう。無論「医者の不養生」と言う言葉を知らない人はいないでしょう。自分、又は自分の部下、の健康管理がそれほど出来ないものは説得力のある健康指導に務められない。
「診察」の概念も流れ作業と勘違いされているかもしれない。辞書によれば「【診】: {動}みる。みおとしのないようにすみずみまでみて、その事がらについて判断を下す。よくみる。」がある。だが何かを「よく」みたいならば、それなりの時間をかけることが必要です。現在実際の状況は異なっても、且つで日本の医療に強い影響を及ぼしたドイツでは「外来診療」を “Sprechstunde” と言う。直訳では「話す時間」です。「財源不足」に悩まされている日本に於いても即検査やハイテックの駆使に走る事を一旦後回しにして、再びこの「良く診る、ゆっくり話す時間」の原点に戻るとよい。時間を掛けて良く診る事は殆どの伝統医療の一つの特徴でもある。
又、上記に「小児科」と言う例を上げた西洋医学領域は多数の「専門分野」に分けられ、そして更に細分化する傾向がまだまだ続く。「専門家」がいることは当然に頼もしいと必要ですが、専門の事しかしないなら視野が大変狭くなり、冒頭に記載したWHOによる健康の定義に基づく保健診療は難しくなる。ある患者の実話によると「新生児の孫が風邪ひいたらしいから開業小児科に連れたが、そこで新生児を診察できないから、大病院に行くように言われた。」
経験と「勘」対EBM、技術的なリソース

人材の他に技術的や知能的なリソースにも無駄の部分が多い。左記のヘッドラインにはそれなりの根拠があるけれども、「進歩」と言う概念(信念?)に視野が塞がられ、医療の原点である触診などが軽視あるいは廃止されると、診察の際即に高価の技術を利用する事になる。矢張り患者の実話ですが、肩の痛みを訴えて病院で診察を受けたら、医師が触診もせず、MRI検査を注文した。触診でその病態が凡そ分かってしまうが、点数が全くあるいは僅かにしか請求できないので、患者の自己負担でさえ2-3万円掛かる検査は日常の臨床の基本になると、保険制度の崩壊は目に見える。ハイテックの画像診断機器や高度の技術を要する検査方法を利用することだけでは、その医療体制が本当にに「発達した」とは言えるでしょうか。
情報及びコミュニケーション 

歴史的の背景によって日本に於いて医者-患者の独特の関係を築いたが、その時代の終止に向かっている気配はある。

医者は基本的「職人」であるにも拘わらず、「医者様」と呼ばれる事決して珍しくない。そうすると医者が患者より「偉い」と言う感覚で診察が行われる。つまり、患者と医者は同レベルの人間ではなく、医者の地位は患者より上から上下関係になる。だがどの上下関係においても「下」の者は「上」の者に対してある程度遠慮する。つまり、外来における医者の質問「如何ですか」に対して患者が「おかげさま」と答えるシナリオは誰でも知っている。だがそれで医者に診察に必要な情報が十分提供されない。
医者は患者が診察の際同時に他の治療も受けているかどうかと聞かれる患者は多分全国的にも少ない。例え「はい」と答えたら、どんな先生はどう言う治療を施しているかを尋ねることは滅多にないに違いない。左記のヘッドラインにも拘わらず医者同士のコミュニケーションは本当に乏しい。これは先進カ国の高度発達した医療制度の本当の姿なのか。そして治療効果の判定は当然「自分」が施している治療のみによるものだと思われ危険が高い。
一人の患者に多数種の薬を処方されるのも一般的ですが、それぞれの薬品が認可されるために行われる臨床試験において大体一種の薬しか検討されない。薬物相互作用に関して2種、多くて3種までが調べられる。同時に8種や10種、場合によって異なる医療機関に重なるような薬を処方される方においてこの組み合わせはこの患者に於いて本当に安全かどうか誰も知らない!これこそ先進国が目指しているEBM (evidence based medicine) で示されている目標より遅れているかを証明している。

また、最近「自然」或いは「漢方」もブームとなっているように見受ける。当然、医療体制はこれを商売のチャンスとして見逃すことは出来ないので、多数の医療施設に「漢方処方」を宣伝し、厚生省はおよそ120種の漢方薬を保険診療のために認可した。製薬会社はそれらの薬の使用目標を手帳にまとめ、病名別や症状別に漢方薬を選択、使用できるようになった。だが漢方薬の使用にあたって漢方医 学独自の概念があって、それを無視すれば本来の漢方薬の良さは発揮できなくなる。6-7年程前に「少柴胡湯」と言う漢方薬が慢性肝炎を目標として使われた際、数人の患者が死亡した事件もあった。それ以来厚生省は漢方薬は危ないと危機を感じ、例の漢方処方の説明書にその危険を赤文字で示されるようになった。しかし、それは漢方薬が危ないではなくて、その使い方を完全に無視している医者が悪い。そこで又上記のヘッドライン(広告)はこの国がいかにも遅れていることを物語っている。東洋医学の1300年の伝統を無視してたった150年で医療現場を制覇し、オールマイティだの現代医学として「日本初」は随分お粗末の気がする。
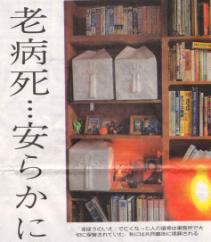
この写真はある施設についての記事にあった。この施設は特に裕福ではない方の世話をしていたそうです。施設の職員も頑張っているに違いないが、私は外国人としてどうしてもその「安らかに」とお骨の上に置いてある娯楽ビデオと横にあるビジネス電話帳のコントラストに驚愕した。スペースはいくら限られているにしても、これが余りにも情けないです。多分第三世界では死者に対してもう少し品のある態度を取るではないでしょうか。
- お骨の上に娯楽ビデオ、その横にビジネス電話帳
この写真はある施設についての記事にあった。この施設は特に裕福ではない方の世話をしていたそうです。施設の職員も頑張っているに違いないが、私は外国人としてどうしてもその「安らかに」とお骨の上に置いてある娯楽ビデオと横にあるビジネス電話帳のコントラストに驚愕した。スペースはいくら限られているにしても、これが余りにも情けないです。多分第三世界では死者に対してもう少し品のある態度を取るではないでしょうか。
お骨の上に娯楽ビデオ、その横にビジネス電話帳
結語
現代医学という表現は略イコール「西洋医学」と使われ,この領域に於いて目覚しい進歩が続き、20年前に夢にも想像できなかった技術で今まで不可能と思われたものを可能にするつつある。しかし、同時に進む「専門化」によって視野が極めて狭い「専門馬鹿」も増えている。受診すると臓器や病症ごとに取り扱われ、その医療体制は機械化して来た。「部品交換」や「修理」される患者には骨の髄まで凍りそうな冷たいものだ。
一方、世界中のどの文明で、どの時代にもあった包括的な医療体制は局所のみではなくて、人間を見る温かいものだ。緊急事態や診断技術などの分野には現代医学の代わりにはなれないが、これらの伝統的な手段は国の財源不足の解消に貢献できる上に国民の知的財産でもある。健康管理は完全に専門家に任せるべきではない。医療従事者の第一の使命は患者を病気から守って、そして病気に掛かった場合出来る限り早くまた自立させることだ。残念ながらこの「理想」は今の時代に「利益」の信念に負けているようです。
日本において東洋医学1300年の歴史あるので、本来この分野で世界のリーダーでもあるべきだが、情報発信地として全くと言えるほど機能していない。上記のWHOが発行の本は日本語に翻訳されているが、WHOの正式のホームページに日本語翻が記載されていない。他の言語はある。中国は世界的レベルで東洋医学思想を支配されているようだ。日本独自の業績でさえ海外では当然のように中国の発想だと思われることが多い。そして、伝統医学と保険の問題や科学的な研究等などに関しても日本はアメリカを見て、真似てしまうことが目立っている。
それでも日本は先進国といえるでしょうか。