he entire human race uses “language”, with the exception of the comparatively few people suffering from some sort of impairment, as a matter of course. Although there are differences regarding region/land and historical time, people in a specific location and at a specific time take the use of their “native” language for communication with other people of the same time and region for granted. While there are differences among different languages in the way how certain things/concepts are handled, the basic idea of conveying information between people is probably everywhere the same.
To quote from the Wikipedia(1):
“(language as) A tool for communication
Yet another definition defines language as a system of communication that enables humans to cooperate. This definition stresses the social functions of language and the fact that humans use it to express themselves, and to manipulate things in the world.”
Again from the Wikipedia, pertaining to communication(2):
“Human communication
Human spoken and written languages can be described as a system of symbols (sometimes known as lexemes) and the grammars (rules) by which the symbols are manipulated. The word “language” is also used to refer to common properties of languages. Language learning is normal in human childhood. Most human languages use patterns of sound or gesture for symbols which enable communication with others around them.”
Problems arise, when people of one specific region try to communicate with people in or from other regions. These problems arise already during communication related to common things like food, housing, directions etc., occasionally even among speakers of different dialects of the same language, but become much more complex in areas of high specialization. Oriental medicine is one such area. Even if one assumes, that the people who try to study and/or communicate about oriental medicine are already experts in their field, communication of specific concepts using different languages may represent a very challenging task. Assuming that there is a wealth of valuable information, which I will define for the sake of this discussion as information originating in Japan, this is and remains of very little use. That is because it is (encrypted) in Japanese, which mainly precludes access to it by most people of the world and information becomes only then really useful, if it is made available/accessible.
I am not a scholar and do not speak on behalf of any particular group of people or organization, but would like to formulate a few of my personal concepts related to this topic. In particular I would like to focus on aspects of the Japanese language, how it seems to be currently handled and understood in this field of learning and what potential future students of oriental medicine might expect or would like to see.
xxxxxxxxxxxxxxxxxxxxxxx
As stated above, language is used to convey concepts among people. This is an extremely simplified statement, but since I do not want to/can delve into all the complexities of research into language, communication and information exchange, I would appreciate, if you will permit me to leave it standing as it is.
The Japanese language is quite different from both English or other European languages and other oriental languages like Chinese. It does not use articles, rarely distinguishes between plural and singular and handles nouns and verbs differently from the way this is done in English for example(5). This may contribute to the impression, that Japanese is complicated and so difficult to learn, that most foreigners are not expected to have much success. Yet, Japanese is a highly developed, delicate and elegant language. Examples of highly refined typical Japanese literature like the “Genji Monogatari” for example, even though they use the writing system imported from China, antedate comparable works sometimes almost by centuries.
Yet, the Japanese people themselves seem to suffer from an inferiority complex about their language precisely because it seems to be so difficult and inaccessible. In a very illuminating book written by the linguist Suzuki Takao “The World of the Closed Language Japanese”(8) the author points out, that Japanese is actually one of the top 10 most spoken languages of the world. In his book he cited Japanese to be on rank 6, but while the rank has dropped to “9”(6) since its publication 30 years ago, it still remains among the most frequently, widely spoken languages of the world. There is nothing to be ashamed (shame is also a concept of special cultural significance in Japan) of. Rather on the contrary: I firmly believe that Japanese people should take more pride in their language and their achievements, which are largely expressed through this language. This in turn suggests, that materials explaining these achievements should be made assessible to the world through translation.
However, because of their fear, that other people/languages may be superior to their own and in conjunction with the aggressive promotion of a “standard TCM terminology” by the Chinese through the WHO(7), the Japanese have adopted a quite restrained behavior of promoting/displaying their own concepts and practice of oriental medicine through the use of Chinese dominated language. The result is an almost unbearable mixture of expressions, circumscriptions etc. that make even comparatively simple ideas almost unintelligible for many students of the matter throughout the world. I will try to illustrate with a few examples.
Occasionally I translate Japanese articles meant for magazines etc. that have the purpose of promoting the Japanese concepts pertaining to the use of Chinese herbal medicine, called Kampo, as well as research into acupuncture and oriental medicine in a wider sense.
Yet, while the use of Chinese herbal medicines in the Japanese way = Kampo should be considered an original Japanese application, editors sometimes/often cling to the Chinese form of an alphabetical notation of the relevant terms. For example, certain editors follow the recommendations by an authoritative academic (Japanese) society for the research into Kampo medicine and thus demand from me, that I write the name for prescriptions as ONE word, appearing in third place after English and Chinese like:
* Cassia Twig and Tuckahoe Pill plus Coix Seed
* Gui-Zhi-Fu-Ling-Wan-Liao-Jia-Yi-Yi-Ren
* keishibukuryoganryokayokuinin
Here I can understand the use of an English translation. That certainly facilitates access to this information. The Chinese notation at least shows the breaks between individual characters, facilitating search in dictionaries and possibly also provides clues about the pronunciation. While the Japanese … (12)
The above shown Japanese “word” has 29 (!) characters. There are even longer ones, like for example “yokukansankachinpihangegotokishakuyakusan” with no less than 41 characters. And, while the English and Chinese terms are treated as proper nouns and thus capitalized, in the example above the Japanese term appears only in lower letters, as if it were no proper noun.
I once asked a scholar about the necessity of expressing the Japanese terms as single words. The answer was, it would be very difficult to decide where to put any possible breaks. Again, I have great difficulties in believing, that the current approach will facilitate the declared purpose(9) of disseminating relevant information.
For example, one could easily break down the expression for the prescription called “Keishikaryukotsuboreito” in the following way:
* Keishi = drug name
* Ka = processing instruction
* Ryukotsu borei = names of TWO drugs
* To = drug form.
Not even Japanese persons would consider Keishikaryukotsuboreito” to be ONE word, even if it is ONE name. For a Japanese person the term becomes immediately intelligible by looking at its elements, in particular since the Japanese know the associated Chinese characters for this term. This latter information and the underlying structure is presumably NOT available to many possible students of the material, unless they have previously acquired a considerable knowledge of the Japanese language, and thus makes comprehension very difficult, it not impossible. This includes also the difficulties encountered during attempts of looking up the term in dictionaries, that are newly created by this notation.
When I showed terms like “ryokeijutsukantogotokishakuyakusan” to Japanese people and asked them to read that for me, ALL were struggling very hard or could not figure it out at all, although they could read, naturally, the term when it is written in Chinese characters.
A little search about the use of long words in the English language showed, that the longest non-coined and nontechnical word is “Antidisestablishmentarianism” with 28 characters and the longest word in Shakespeare’s works is “Honorificabilitudinitatibus” with 27 characters(4). So, for any “reasonable” discussion words of less than 20 characters should be suitable/comprehensible. “yokukansankachinpihangegotokishakuyakusan” (41 characters) is simply incomprehensible. The use of notations like “Thisisalonggreenhouseattheroadside” or “Lelangageestunsystme de signesidentifis permettantunecommunication entreune ouplusieursentits” would NOT help any learner of English of French respectively. Further, I believe that MOST people will have difficulties pronouncing the English word “Supercalifragilisticexpialidocious” with 34 letters, that was in the song with the same title in the Disney musical film Mary Poppins(10), without any practice.
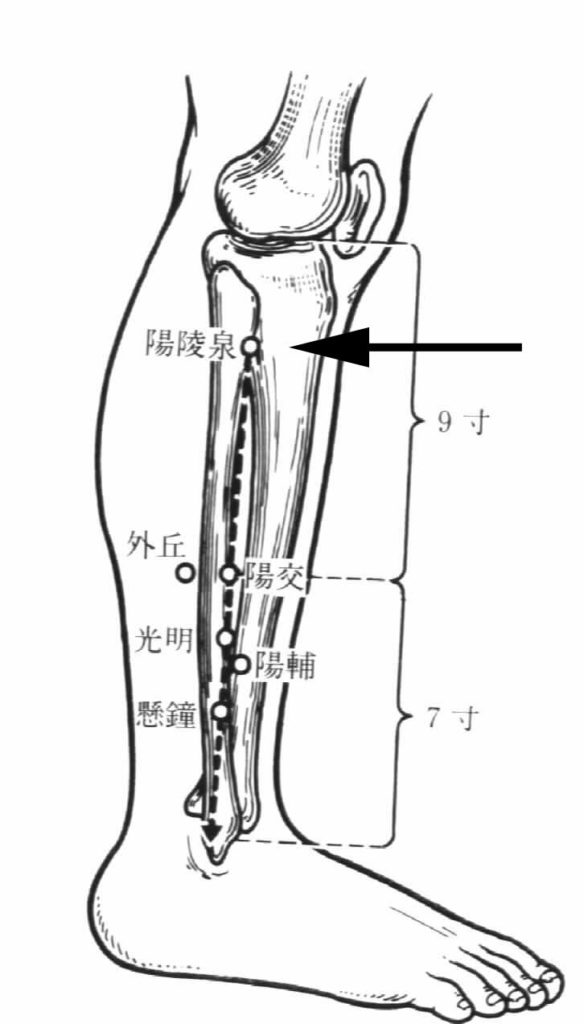
Following the same argument, I think it would help both foreign students as well as ultimately also the Japanese practitioners, if terms related to acupuncture like “Seppi”, “Hinai Shin” etc. were left in Japanese and maybe provided with a descriptive English translation. In a similar fashion the technical terms related to Judo or other forms of martial arts are used WITHOUT translation. If the provision of such word pairs is too difficult to integrate into every text, it should be no problem at all to set up a frequently updated online database with the relevant terms.
After all, anyone who starts learning a certain subject, here oriental medicine, or a particular language, here Japanese, WILL have to refer to dictionaries and other reference materials. In this respect, with all due deference, I am under the impression that the highly educated scholars who have apparently been working on the above mentioned standard terminology or are representatives of the academic societies that strive to study oriental medicine and disseminate the relevant information, may have lost touch with basic problems learners have to face. In particular regarding the use of terminology, I firmly believe that the currently used Japanese approach is wrong.
Let’s consider the use of dictionariess for an attempt to find out more about “keigairengyoto” = Jing-Jie-Lian-Qiao-Tang.
If you use a Chinese-English dictionary that provides alphabetized entries, you will know, that you are looking at a term consisting of 5 characters and can look up each according to its reading. However, there are naturally a large number of characters reading “Jing” and in ordinary language most probably no combination like “Jing-Jie”. For that purpose you need a special dictionary.
The Japanese is worse, much worse. Here you are offered only ONE term. Even if the learner suspects, that this term consists for more than one character, HOW should this learner look for the relevant characters? The term could be split like:
* ke iga iren gyo to
* kei gairen gyoto
* keiga iren gyoto
* keigai rengyo to etc.
That gives the student many possible dictionary entries to look up – a largely futile effort.
For anyone who does not know the language (Japanese), all of the listed divisions are equally possible. Depending on how the individual terms/characters are listed in the particular dictionary, this may render a search almost impossible. If the particular dictionary does NOT provide alphabetized notations, most foreign readers are denied access to this information right from the start. I have experienced this myself many times. Unfortunately, to my knowledge there are, with one little exception(11), no proper dictionaries that would help foreign students getting access to the required information. The shortest, and only, way would always require the combined use of several Chinese-English, Chinese character, Japanese-English dictionaries. Occasionally more than one of each type.
Apart from the standard dictionaries there are a number of special dictionaries for oriental, in this context mostly Chinese medicine. Sometimes the tycoons in the field publishing those dictionaries then argue about who has the “right” translation, which will invariably be different from what is found in dictionaries published in China and among the latter ones again, each gives something different and here the English rendition itself more often than not appears to be rather dubious. What the WHO has published recently as the “agreed upon standard terminology” still feels in many instances not right, at least to me. And, naturally, that terminology assumes that everything must be based on Chinese concepts.
Since people are basically dealing with “Chinese medicine”, this consensus is of course not wrong, but what happened to the Japanese view and all those aspects special to Japan? The basic concepts of acupuncture and herbal medicine have been brought to Japan about 1,500 years ago and over centuries after that through books and by practitioners. Yet, that is a long enough period for some original, independent developments to take place. Take for example the use of guiding tubes for acupuncture: a purely Japanese invention. In conjunction with the cultural differences, climatic and geographic differences and not least the mentality of the people this period of 1,500 years of development has led, I believe, to the establishment of conceptional systems and practical applications that are clearly distinct from the Chinese form ? even though many Japanese practitioners strongly assert, that they are practicing CHINESE medicine.
In spite of the thus historically formed system of a typical Japanese approach to oriental medicine, the insistence of the people in charge to NOT make this information publicly known, or to choose deliberately expressions/notations that are/will be incomprehensible for many/most non-Japanese persons, is a waste of very valuable resources.
I do hope, and possible can help to stimulate the process to adopt a more enlightening approach to the “dissemination of information”, so that the mountains of intellectual treasures currently hidden behind the veils of the Japanese language can be more easily assessed by the people of the world.
References:
(1) http://en.wikipedia.org/wiki/Language
(2) http://en.wikipedia.org/wiki/Communication
(3) http://en.wikipedia.org/wiki/Information
(4) http://en.wikipedia.org/wiki/Longest_word_in_English
(5) An Introduction to Japanese Syntax, Grammar & Language
by Michiel Kamermans; grammar.nihongoresources.com
http://grammar.nihongoresources.com/doku.php
http://www.thejapanshop.com/
(6) http://en.wikipedia.org/wiki/List_of_languages_by_number_of_native_speakers
http://www.photius.com/rankings/languages2.html
(7) WHOIST
WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region
(8) 鈴木孝夫: 閉ざされた言語・日本語の世界 (Suzuki Takao “The World of the Closed Language Japanese”)
(9) From the JSOM HP:
“Objective:
The intention of the society is to hold research presentations and seek communication, tie-up and promotion concerning oriental medicine and contribute to the progress and dissemination of oriental medicine, and thus contributing to the development of scientific culture.”
(10) http://en.wikipedia.org/wiki/Supercalifragilisticexpialidocious
(11) Japanese-English Dictionary of Oriental Medicine; written and compiled by JONG-CHOL CYONG M.D. & Ph.D.; Oriental Medicine Research Center of the Kitasato Institute, Tokyo; ISEISHA
(12) Comment pertaining to: “WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region”:
* In this dictionary the items are listed in the order “Code ? Term ? Chinese ? Definition/Description”. “Term” represents the column with the English terms and “Chinese” lists the corresponding Chinese terms ONLY in Chinese characters. That means, users cannot search the dictionary according to reading/pronunciation of Chinese terms and MUST know, what they are looking for in English. Or else they have to read through entire sections of the book.
* The only section, that provides “pronunciation” is the one listing classical medical texts. However, this too looks to users who are NOT very familiar with the different involved languages like a deliberate attempt at making things as incomprehensible as possible:
Chinese: 素問玄機原病式 = Suwenxuanjiyuanbingshi
“Suwen” may be known well enough, but xu-an-ji or xuan-ji?
Japanese: 百腹圖説 Hyakufukuzusetsu
Should it be “pronounced” Hyakufu kuzu setsu or Hya kufu ku zusetsu?
萬安方 Man’ampo ? the approstrophe is almost a relief and very helpful!!!
Korean: 鄕藥救急方 Hyangyakgoogeupbang ? I have no idea at all how this is supposed to be pronounced!
Vietnamese: 保嬰良方 Bao Anh luong phuong ? even though I do not know how to pronounce that, I can clearly infer, that the term is made of 4 characters and look up their respective meaning, if I have Vietnamese dictionary (with alphabetical notation).
Even if the above are ‘single terms’, I am convinced that native speakers of the respective language pronounce these terms with certain intonational structure, revealing the listener clues to the makeup of the relevant terms. Without these clues, in the above example the apostrophe shows the listener/reader, that there is a break after “Man” and the term is not read Manam Po. Considering that even native speaker among themselves use these intonational structures, imagine what will happen, if someone who does not know the proper pronunciation of the relevant languages tries to read those terms / pronounce them / use them during communication with other practitioners.